Approximately 1.2 million individuals in the US are living with HIV.1 Due to the advent of modern antiretroviral therapy, patients with HIV are living longer. In 2021, it was estimated that nearly two-thirds of individuals with HIV in the US were age 45 years or older.2 Although antiretroviral therapy that durably suppresses HIV replication is of utmost importance, as the HIV population ages, treatment of co-morbid conditions must be addressed.
Research has well established that individuals with HIV are at higher risk of cardiovascular disease. For example, studies have reported anywhere from 20% to 100% increased risk of myocardial infarction in this patient population.3 Unfortunately, this risk persists despite well-controlled HIV. The mechanisms behind the increased risk of cardiovascular disease are still being studied. However, current hypotheses include persistent inflammation and immune activation; CD4-positive cell depletion; exposure to older, toxic antiretroviral therapies; and traditional risk factors such as diabetes, smoking, and poor dietary habits. Until recently, there was no specific guidance for prevention of cardiovascular events in patients with HIV. Given the results of the recently published REPRIEVE trial (NCT03455390), health care providers now have data specific for this important patient population.
The phase 3 Randomized Trial to Prevent Vascular Events in HIV (REPRIEVE)4 enrolled 7769 participants with HIV infection between 40 to 75 years of age with low-to-moderate risk of cardiovascular disease who were receiving antiretroviral therapy. Treatment was randomly assigned with 4 mg daily pitavastatin calcium (Livalo; Kowa) or placebo. Pitavastatin calcium was chosen because it does not interact with the drugs that are used in antiretroviral therapy.4
The primary outcome was the occurrence of a major adverse cardiovascular event (MACE), including cardiovascular death, myocardial infarction, hospitalization for unstable angina, stroke, transient ischemic attack, peripheral arterial ischemia, revascularization of a coronary carotid or peripheral artery, or death from an undetermined cause as measured in a time-to-event analysis. A key secondary outcome was a composite of a MACE or death from any cause.4
The median age was 50 years, 65% were non-White, and 31% were women. Median screening low-density lipoprotein cholesterol (LDL-C) level was 108 mg/dL and median CD4-positive count was 621 cells/mm3. The median 10-year Atherosclerotic Cardiovascular Disease risk score was 4.5%, and 83% of participants remained in follow-up with 74.8% in the pitavastatin group and 71% in the placebo group continuing to receive their randomized treatment at the time of the report. Treatment discontinuation rates due to adverse events were similar at 2.1% and 1.2% in the pitavastatin and placebo arms, respectively.4
The trial was stopped early for efficacy after a median of 5 years due to a 35% reduction in MACE and 21% reduction in MACE or death in the pitavastatin group. A combination of statin and antiretroviral therapy may provide further benefit in reducing cardiovascular disease risk. Although the results are specific to pitavastatin, other statins may have similar protective effects.4
Due to the efficacy found in the REPRIEVE trial, the Department of Health and Human Services/National Institutes of Health HIV Clinical Guidelines updated their recommendation to include that all individuals with HIV to aged 40 to 75 with at least a 5% atherosclerotic cardiovascular disease risk should receive a moderate-intensity statin.5 Because nearly two-thirds of individuals with HIV are at least 45 years old,2 the recommendation to initiate a moderate-intensity statin for those aged 40 to 75 is applicable to most people living with HIV.
About the Authors
Sara B. Jeter, PharmD, BCIDP, AAHIVP, is an HIV clinical pharmacist at University of Kentucky Healthcare.
Jarrod Coffey, PharmD, AAHIVP, is principal medical scientist of HIV at Gilead Sciences, Inc.
Katy L. Garrett, PharmD, BCIDP, AAHIVP, is a medical scientist of HIV at Gilead Sciences, Inc.
The authors wish to thank Dr. Carl Fichtenbaum for his assistance with table creation.
Pharmacists are uniquely apt to help implement these recommendations, regardless of practice setting. Those in HIV-focused clinical settings, primary care, inpatient, retail, and beyond all play a role in improving patient health. In many of these settings, proactive chart review to ensure appropriate statin use is already a standard practice; the patient population that qualifies has simply expanded. In other settings, medication therapy management reimbursement can be a driving factor to work toward statin implementation in this patient group. At every patient encounter, whether at admission or when dispensing a refill, pharmacists can broach statin use when indicated and assist with appropriate statin selection. Antilipidemic agents are the second-most prescribed class of medication,6 so pharmacists are also used to navigating insurance claims, formulary substitutions, and providing appropriate counseling for these agents. This can allow for a seamless transition to beginning a statin or switching to a more appropriate option.
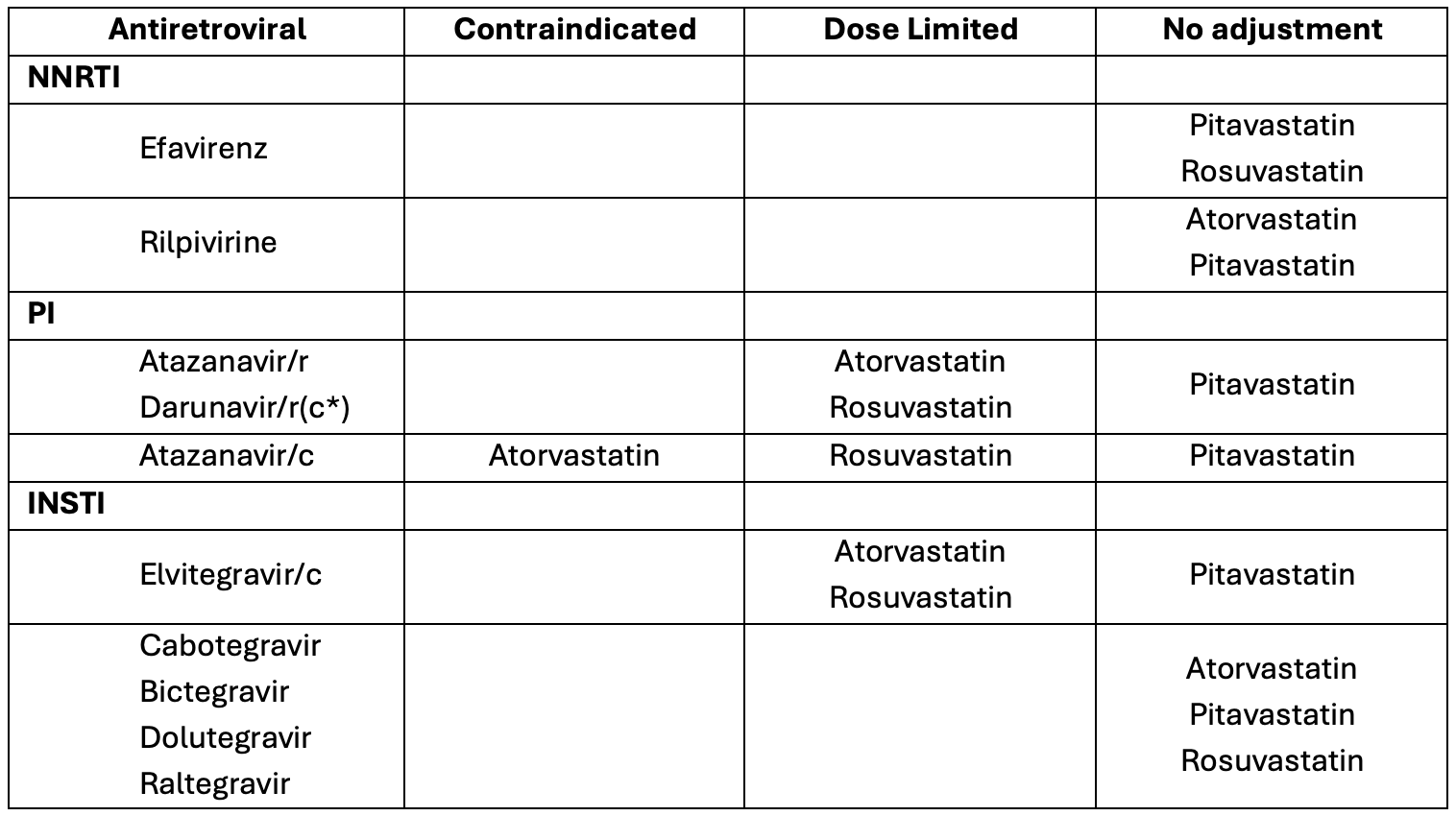
When selecting the appropriate statin, it is important to know the pharmacokinetics of both the statins and the antiretrovirals to assess for any potential adverse events that could be mitigated. Tables 15,7 and 25,7 below list the commercially available statins, stratified by LDL–lowering intensity. Atorvastatin 20 mg, pitavastatin 4 mg, and rosuvastatin 10 mg are the guideline-recommended statins and doses based on data from REPRIEVE. Therefore, any potential drug-drug interactions between them and commonly used antiretrovirals are listed.
Individuals with HIV are living longer lives and have an increased risk of cardiovascular events. Recently published REPRIEVE data have influenced guideline changes to incorporate statin use more broadly. A moderate-intensity statin is now indicated for most patients with HIV, and pharmacists are poised to help implement these changes and improve cardiovascular outcomes for their patients.
REFERENCES
1. Centers for Disease Control and Prevention. HIV Surveillance Supplemental Report: Estimated HIV Incidence and Prevalence in the United States, 2018–2022. Revised May 21, 2024. Accessed May 23, 2024. https://stacks.cdc.gov/view/cdc/156513
2. Sullivan PS, Woodyatt C, Koski C, et al. A data visualization and dissemination resource to support HIV prevention and care at the local level: analysis and uses of the AIDSVu Public Data Resource. Journal of medical Internet research. 2020;22(10):e23173.
3. So-Armah K, Benjamin LA, Bloomfield GS, et al. HIV and cardiovascular disease. Lancet HIV. 2020;7:e279-93. doi:10.1016/S2352-3018(20)30036-9
4. Grinspoon SK, Fitch KV, Zanni MV, et al. Pitavastatin to Prevent Cardiovascular Disease in HIV Infection. The New England journal of medicine. 2023;389(8):687-699. doi:10.1056/NEJMoa2304146
5. Department of Health and Human Services. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Revised February 24, 2024. Accessed May 23, 2024. https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv
6. Santo L, Kang K. National Ambulatory Medical Care Survey: 2019 National Summary Tables. doi: https://dx.doi.org/10.15620/cdc:123251
7. Ecker RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;25(2):S76-99. doi: 10.1161/01.cir.0000437740.48606.d1