|Articles|October 3, 2022
Explore Novel Treatment Modalities for Mantle Cell Lymphoma
Author(s)Jeremiah Moore, PharmD, BCOP
Two recent clinical trials highlight the novel therapy options available to patients in the upfront and relapsed settings.
Advertisement
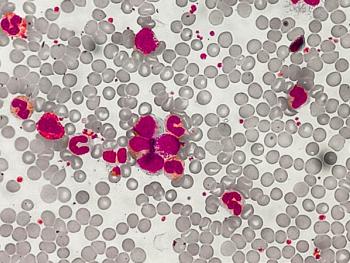
Mantle cell lymphoma (MCL) is a rare type of B-cell non-Hodgkin lymphoma (NHL) characterized by the t(11;14) translocation, resulting in cycle D1 overexpression.
The median age of diagnosis ranges between aged 60 and 70 years and is more common in males.1,2 MCL is generally aggressive, with patients often diagnosed with advanced stage disease, lymphadenopathy, and bone marrow involvement.1,3
Standard upfront treatment for younger and fit patients includes induction chemo-immunotherapy, followed by consolidation with autologous stem cell transplant and rituximab maintenance. Older and less-fit patients receive induction therapy with less aggressive chemo-immunotherapy with or without rituximab maintenance. MCL is an incurable disease, and most patients relapse. In the relapsed setting, treatment options include Bruton’s tyrosine kinase (BTK) inhibitors (acalabrutinib, ibrutinib, zanubrutinib), lenalidomide-rituximab, and chimeric antigen receptor T-cell (CAR-T).3
Two recent clinical trials (ZUMA-2 [NCT04880434] and SHINE [NCT01776840]) highlight the novel treatment options available to patients in the upfront and relapsed settings.
SHINE, a multi-centered, phase 3, randomized trial, evaluated the addition of ibrutinib to bendamustine-rituximab (BR) in the upfront treatment of MCL. Patients aged 65 years or older were randomized in a 1:1 ratio to 6 cycles of BR, with or without ibrutinib 560 mg daily, those achieving a partial response or better continued placebo/ibrutinib plus rituximab maintenance. The primary endpoint was progression-free survival (PFS) as assessed by the study investigators. With a median age of 71 years, 523 patients were randomized, 261 in the ibrutinib group and 262 in the placebo group. PFS was 80.6 months in the ibrutinib group vs 52.9 months in the placebo group (HR 0.75; 95%CI 0.59-.96, p=0.01).4 No new safety concerns were noted with the combination of BR and ibrutinib. The addition of ibrutinib therapy significantly increased the PFS when given in combination with BR.
Because many patients with MCL are older and/or not candidates for upfront treatment options, novel treatment approaches are needed. The results of the SHINE trial showing a PFS difference of >27 months are remarkable.
The ZUMA-2 trial, a multi-centered, open-label, phase 2, single-arm, study evaluated the anti-CD19 CAR-T therapy KTE-X19 in relapsed or refractory MCL patients. Eligible patients needed to be ≥ 18 years of age and received MCL directed therapy, including anthracycline or bendamustine chemotherapy, anti-CD20 monoclonal antibody, and BTK inhibitor therapy. The primary endpoint was the objective response rate (ORR), as assessed by an independent review committee. Seventy-four patients enrolled, with 68 receiving KTE-X19 therapy. The median age was aged 65 years, and 81% had received ≥3 lines of therapy. Sixty patients were included in the primary analysis showing an ORR of 93% and a complete response rate of 67%.5
Based on the results of the ZUMA-2 trial the FDA approved brexucabtagene autoleucel (Tecartus) for patients with relapsed or refractory MCL. Brexucabtagene autolecuel carries a black box warning for cytokine release syndrome and neurological toxicities and is available through the Tecartus risk evaluation and mitigation strategy (REMS) program.
BTK inhibitor therapy for relapsed/refractory MCL is standard of care. the SHINE trial highlights the potential benefit of incorporating this class of medication into the upfront setting. Limited treatment options exist for patients who have not been successful using BTK inhibitor therapy. The results of the ZUMA-2 trial show the promise of CAR-T therapy for this patient population.
Conclusion
The results of the SHINE and ZUMA-2 trials highlight the novel treatment approaches that are being used in the upfront and relapsed MCL settings.
References
1. Armitage JO, Longo DL. Mantle-cell lymphoma. N Engl J Med. 2022;386(26):2495-2506. doi:10.1056/NEJMra2202672
2. Silkenstedt E, Linton K, Dreyling M. Mantle cell lymphoma - advances in molecular biology, prognostication and treatment approaches. Br J Haematol. 2021;195(2):162-173. doi:10.1111/bjh.17419
3. B-cell lymphomas (version 5.2022). National Comprehensive Cancer Network. Accessed July 29, 2022. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf
4. Wang ML, Jurczak W, Jerkeman M, et al. Ibrutinib plus bendamustine and rituximab in untreated mantle-cell lymphoma. N Engl J Med. 2022;386(26):2482-2494. doi:10.1056/NEJMoa2201817
5. Wang M, Munoz J, Goy A, et al. KTE-X19 CAR t-cell therapy in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2020;382(14):1331-1342. doi:10.1056/NEJMoa1914347
Advertisement
Related Content
Advertisement



Latest CME




























































































































Advertisement
Advertisement
Trending on Pharmacy Times
1
NK3 as a Drug Target: From Scientific Discovery to Guideline-Recognized Therapy
2
Sonrotoclax Plus Zanubrutinib Produces Deep MRD Responses in Treatment-Naive CLL
3
Orforglipron Reduces Body Weight Up to 14% in Women at Every Stage of Menopause
4
New Evidence Positions Finerenone as Foundational Therapy Across the CKD Spectrum
5