Take Steps to Prepare for DIR Fee Changes in 2024
Up-front payments to pharmacies will be significantly lower starting this year, creating cash flow challenges
Much ink has been spilled and many “solutions” sold to pharmacy owners and operators regarding the CMS final rule published in May 2022, which dramatically changed the policy landscape for pharmacies that serve Medicare Part D beneficiaries.1 Although much of the commentary surrounding those changes lamented the final rule, pharmacists and pharmacy owners can get prepared and be reassured that their world is not ending.


Image credit: joyfotoliakid | stock.adobe.com

THE DIR FEE LANDSCAPE
Direct and indirect remuneration (DIR) fees are defined by Medicare as any money that a Medicare Part D plan (PDP) or their pharmacy benefits manager (PBM) receives from anybody other than the federal government or the patient.2 DIR, therefore, includes manufacturer formulary rebates, price protection rebates, pharmacy price concessions, audit recoupments, legal settlements, and any other money that a PDP receives. PDPs are required to report to Medicare the total amount of money they received as DIR at the end of each plan year. This is so that Medicare can calculate the amount that the PDP is owed under the financial rules laid down in the Medicare Modernization Act and subsequent statutes that updated the Part D program, including, most notably, the Affordable Care Act (ACA) and the Inflation Reduction Act.1
When pharmacists discuss DIR, they most typically mean pharmacy price concessions, which are a subset of the overall DIR that a plan reports to Medicare. This subset has grown dramatically since the passage of the ACA. In the proposed rule, Medicare reported that pharmacy price concessions had grown by more than 107,000%, meaning they increased by a factor of 1070 times.1 This is unsurprising to anyone who has looked in detail at the financials of a pharmacy.
These incredible increases in DIR paid by pharmacies to PDPs are not accidental and are the direct result of the choices made by CMS in finalizing the 2014 definition of “negotiated price” in its regulations to allow negotiated price to be “inclusive of all price concessions from network pharmacies except those contingent price concessions that cannot reasonably be determined at the point of sale.”3 Under this definition, PBM legal teams and other internal teams quickly devised “pay for performance” programs that allowed them to state, factually, that the price concessions under such arrangements could not be estimated at the point of sale. As a result, today, after 10 years of increasing the effect of such programs, there exists a substantial fraction of prescriptions wherein the PBM collects a contingent performance fee in excess of the total pharmacy reimbursement (eg, the pharmacy collects $5 from the patient as a co-pay, and then the PBM collects $50 from the pharmacy in DIR, for a total negative payment to the pharmacy of $45).3

This situation is untenable for pharmacies and increases the co-payments for older patients, as well as the payments by manufacturers and the federal government, well above what they would be in the absence of the financial fees executed by PBMs and PDPs under this definition of negotiated price.
CHANGES IN 2024
In 2022, CMS changed the definition of negotiated price to mean the lowest possible payment that a pharmacy could receive under any performance program.1 This change is an excellent change to the structure of Medicare Part D because it removes the ability of PDPs to shift costs onto their beneficiaries, the federal government, pharmacies, and pharmaceutical manufacturers.1
However, any major shift in policy that impacts significant funds transfers per pharmacy will have unintended effects. In particular, due to this change, PBMs have restructured their PDP contracts with pharmacies from a structure wherein pharmacies receive a grossly inflated payment and then have to pay that inflated amount back as DIR, to a structure that more closely resembles the commercial market. Under this structure, pharmacies are paid a fairly aggressive up-front amount for the products they dispense, and there is no back-end fee.4
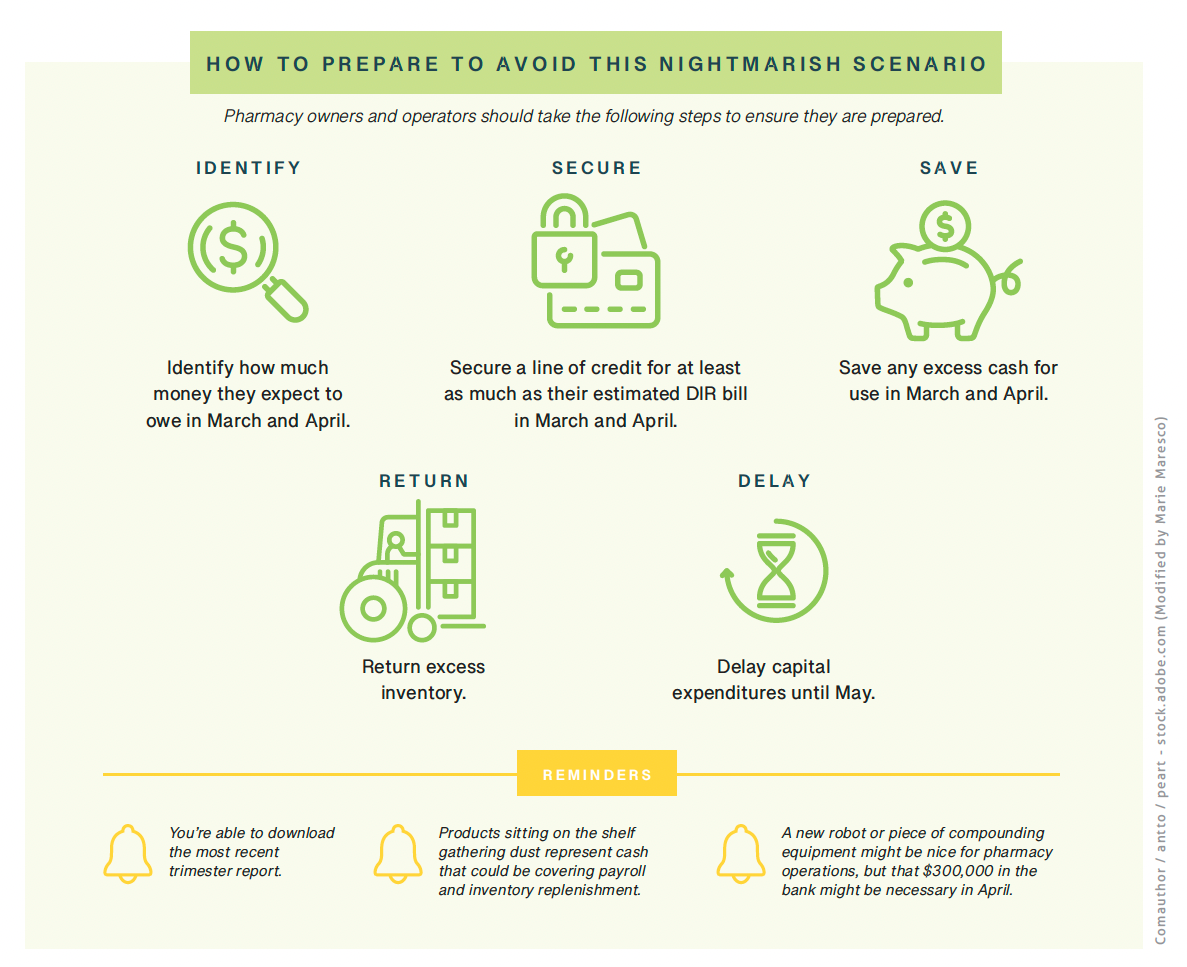
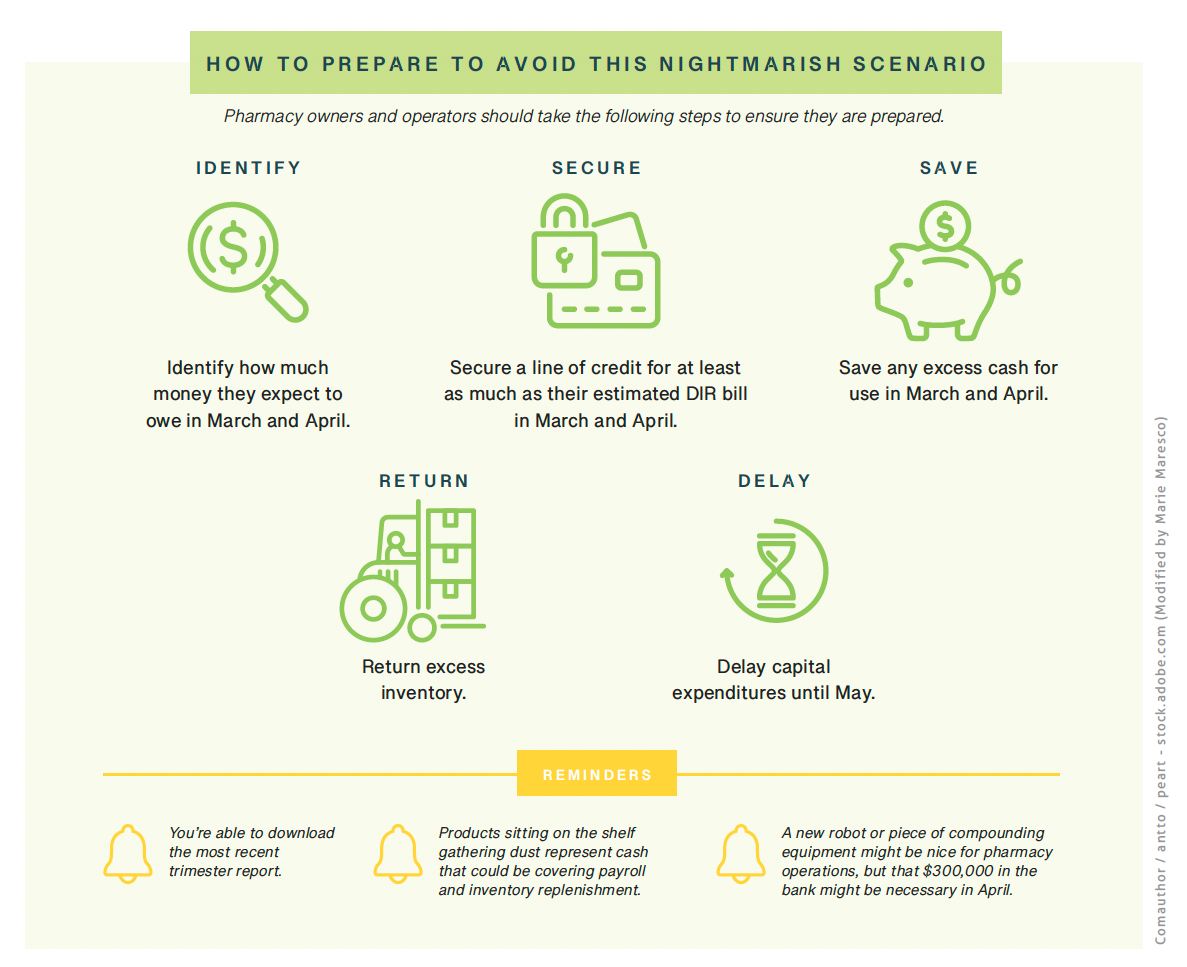
Some PBMs and PDPs have elected to continue to operate contingent performance programs, but those sums will, for the most part, be separate from the up-front claim payment amount. However, because of the structure of CVS Caremark’s current performance program, pharmacies will continue to owe DIR payments to that PBM in March and April 2024 based on claims billed in the last 4 months of 2023.4 Because the up-front payments in 2024 will be much lower (average wholesale price [AWP] minus 18% to 26% in 2024 vs AWP minus 4% to 11% in 20231), this will result in a liquidity crunch for pharmacies. The cash coming in for ongoing business in March and April 2024 will be less, and pharmacies will have to pay CVS Caremark’s DIR fees out of ongoing checks as well,4 which will further reduce cash on hand. Once April 2024 is over, the pharmacies that have planned their expected cash needs will be past the worst cash situations they will likely ever see. However, pharmacies that failed to plan their cash needs will likely be unable to meet their wholesaler bills and payroll.
About the Author
Benjamin Jolley, PharmD, is a pharmacist at Jolley’s Compounding Pharmacy, and the cofounder of Apex Pharmacy Consulting. He can be reached at benjamin@apexpharmacyconsulting.com.
References
- Medicare Program; Contract Year 2023 Policy and Technical Changes to the Medicare Advantage and Medicare Prescription Drug Benefit Programs; Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency; Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency. 42 CFR §417, §422-423 (2022). https://www.federalregister.gov/documents/2022/05/09/2022-09375/medicare-program-contract-year-2023-policy-and-technical-changes-to-the-medicare-advantage-and
- Medicare Part D –Direct and Indirect Remuneration (DIR). News release. Centers for Medicare & Medicaid Services. January 19, 2017. Accessed January 5, 2024. https://www.cms.gov/newsroom/fact-sheets/medicare-part-d-direct-and-indirect-remuneration-dir
- Medicare program; contract year 2015 policy and technical changes to the Medicare Advantage and the Medicare prescription drug benefit programs; final rule. Fed Regist. 2014:79(100):29843-29968. https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/MedicareProviderSupEnroll/Downloads/CMS-4159.pdf
- Hunter E. DIR Fee Reform Will Have Repercussions in 2024, But Pharmacists Can Prepare. Pharmacy Times. July 20, 2023. Accessed January 8, 2024. https://www.pharmacytimes.com/view/dir-fee-reform-will-have-repercussions-in-2024-but-pharmacists-can-prepare