Abstract
As literature and guidelines increasingly support the use of continuous glucose monitoring (CGM) technology, clinicians are implementing it into clinical practice. CGM assists clinicians in overcoming clinical inertia by allowing them to optimize pharmacological therapy while diminishing hypoglycemia risk. However, it may be difficult for clinicians to stay up to date with currently available CGM devices and guideline recommendations. Pharmacists can assist in choosing the ideal CGM device for each candidate, provide training, analyze glycemic trends, and optimize medication therapy based on the data. Pharmacists may also be able to bill for these services to ensure a sustainable practice model. This guide is for pharmacists who are interested in utilizing CGM technology in clinical practice. It discusses differences between personal-use and professional-use CGM devices and features of each CGM device currently available. Additionally, it provides an overview of considerations and candidates, interpretation of reports, coverage, and billing.
Background
Diabetes is a chronic disease affecting approximately 10.5% of the US population.1 Since the mid-1800s, there have been attempts to control diabetes by quantifying glucose in the urine. The first blood glucose (BG) test strip (Dextrostix; Ames) was developed in 1965 and was used at medical offices, but the first glucometer was not created until the 1980s. Over time, glucometers improved and became the standard of care. The first professional CGM was approved by the FDA in 1999.2,3
CGM measures interstitial glucose instead of plasma glucose and records glucose levels every 5 to 15 minutes. Depending on the device, it can be worn for 7 to 90 days. CGM devices are subdivided into personal and professional. Personal-use CGMs are owned by the patient and can be further divided into real-time CGM (rtCGM) and intermittently scanned CGM (isCGM). On the other hand, professional CGM devices are owned by the clinic and are placed on a patient in a medical office for a discrete time period. RtCGM measures and displays glucose levels without scanning. In contrast, isCGM will display only glucose levels scanned by a reader or smartphone and requires scanning at least once every 8 hours to avoid gaps in glycemic tracing.4 Recommendations for CGM are dependent on patient-specific factors and pharmacological therapy.
Proper use of CGM devices will help clinicians, such as pharmacists, manage glycemia. Depending on the state, pharmacists can practice under medication therapy management (MTM), comprehensive medication management (CMM), and/or collaborative drug therapy management (CDTM).5 Determined by state regulations, pharmacists are able to prescribe CGM devices based upon guideline recommendations and provide adequate training to patients and caregivers.
Guidelines
For adults, the 2023 American Diabetes Association (ADA) guidelines recommend that rtCGM (grade A) or isCGM (grade B) be offered to patients on multiple daily injections (MDIs) or continuous subcutaneous insulin infusions (CSIIs). Additionally, adults requiring basal insulin can be offered rtCGM (grade A) or isCGM (grade C). In patients who are pregnant, CGM can be used to achieve hemoglobin A1C (HbA1C) goals (grade B). Youth patients with type 1 diabetes (T1D) who are on multiple daily injection (MDI) or continuous subcutaneous insulin infusion (CSII) therapy should be offered either an rtCGM (grade B) or isCGM (based on expert opinion). For young patients with type 2 diabetes (T2D) requiring MDI or CSII, CGM can also be recommended (based on expert opinion).4
The 2021 American Association of Clinical Endocrinology (AACE) Clinical Practice Guideline: The Use of Advanced Technology in the Management of Persons With Diabetes Mellitus strongly recommends CGM for patients treated with intensive insulin therapy, which is defined as 3 or more injections of insulin per day or the use of an insulin pump (grade A: high strength of evidence). The 2021 AACE Advanced Technology Guidelines recommend CGM to all patients with problematic hypoglycemia, children/adolescents with T1D, and pregnant women with diabetes treated with intensive insulin therapy (grade A: intermediate-high strength of evidence) or gestational diabetes on insulin therapy (grade A: intermediate strength of evidence). CGM may be recommended for women with gestational diabetes who are not on insulin therapy and individuals with T2D on less intensive insulin regimens, including basal insulin monotherapy or noninsulin therapy (grade B: intermediate strength of evidence).6 The updated 2022 AACE guidelines recommend rtCGM or isCGM for all patients with T1D (grade A) and patients with T2D who are treated with insulin therapy or at high risk for hypoglycemia with or without hypoglycemia unawareness (grade A).7 These recommendations are based upon recent literature, which highlights the benefits of CGM.
Literature Review of CGM in T2D
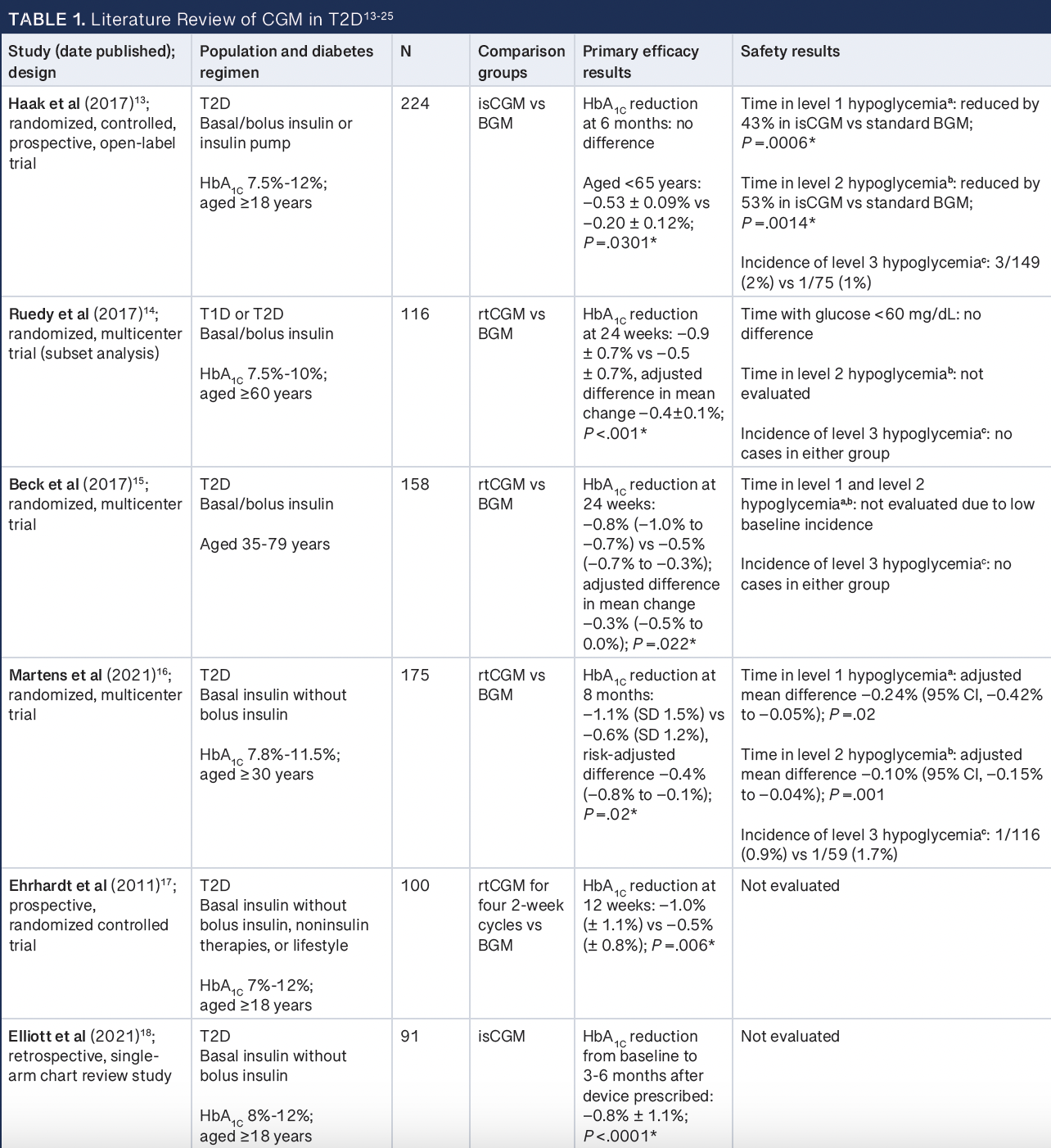
While the benefit of CGM in improving glycemic control and reducing hypoglycemia in patients with T1D has been established, recent literature also supports the use of CGM in patients with T2D.8-12 Similar to patients with T1D, patients with T2D using intensive insulin regimens require BG monitoring (BGM) multiple times per day. Use of both isCGM and rtCGM in those with T2D using intensive insulin regimens has been associated with significant reductions in HbA1C at 6 months compared with BGM.13-15 A study (NCT02082184) by Haak et al utilizing isCGM found a glycemic benefit only in a subset of patients younger than 65 years.13 However, Ruedy et al found that rtCGM use was associated with improvements in HbA1C in a population 60 years or older, suggesting that benefits may span all adult patients.14
In addition to being associated with improved glycemic control, Haak et al found that isCGM use was associated with a reduction in time spent in the hypoglycemic range.13 On the other hand, Ruedy et al and Beck et al did not find an association between rtCGM and a reduction in hypoglycemia in patients using intensive insulin regimens, though rates of hypoglycemia were low at baseline in both studies.14,15 Participants in Beck et al expressed high satisfaction with CGM use and low perceived hassle associated with the device, though there was no difference in change in quality-of-life scores between the groups.15
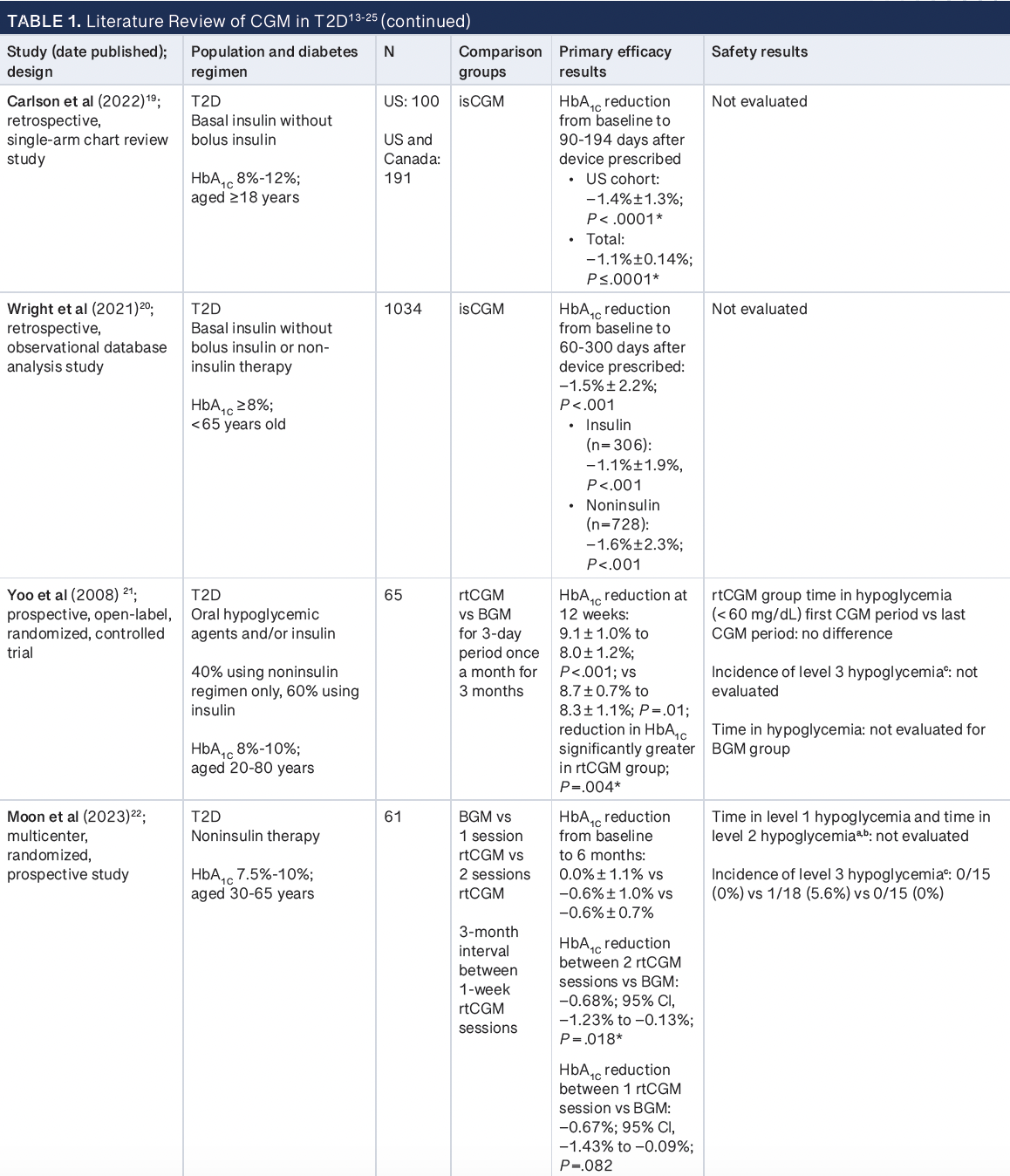
Given the benefits of CGM use in patients using MDI, there has been increasing interest in the use of CGM in patients with T2D using basal insulin and noninsulin regimens. Several randomized and observational studies have found that CGM is associated with HbA1C reductions in those using basal insulin without bolus insulin or noninsulin therapies, with the greatest impact seen in those with the highest baseline HbA1C.16-21 Martens et al found that rtCGM use for an 8-month period was associated with a greater time in range (TIR) compared with BGM (TIR, 59% vs 43%; P < .001).16 The majority of studies in those using basal insulin without bolus insulin or noninsulin regimens did not assess the impact of CGM use on hypoglycemia.17-20 One study (NCT04854135) that assessed the incidence of hypoglycemia or severe hypoglycemia in patients using oral hypoglycemic agents with or without basal insulin did not find any differences in incidence between rtCGM and BGM use.21 An exploratory analysis in another study showed a possible reduction in time below range (TBR) in the rtCGM group compared with the BGM group.16
In addition to glycemic benefits associated with CGM use, it is possible that use of CGM may have an impact on lifestyle modifications in patients on basal insulin or noninsulin agent. While Erhardt et al did not find significant changes in weight associated with rtCGM use, Yoo et al found that rtCGM use was associated with significant reductions in weight and total calorie intake as well as increases in exercise after 3 monthly 3-day periods of use.17,21
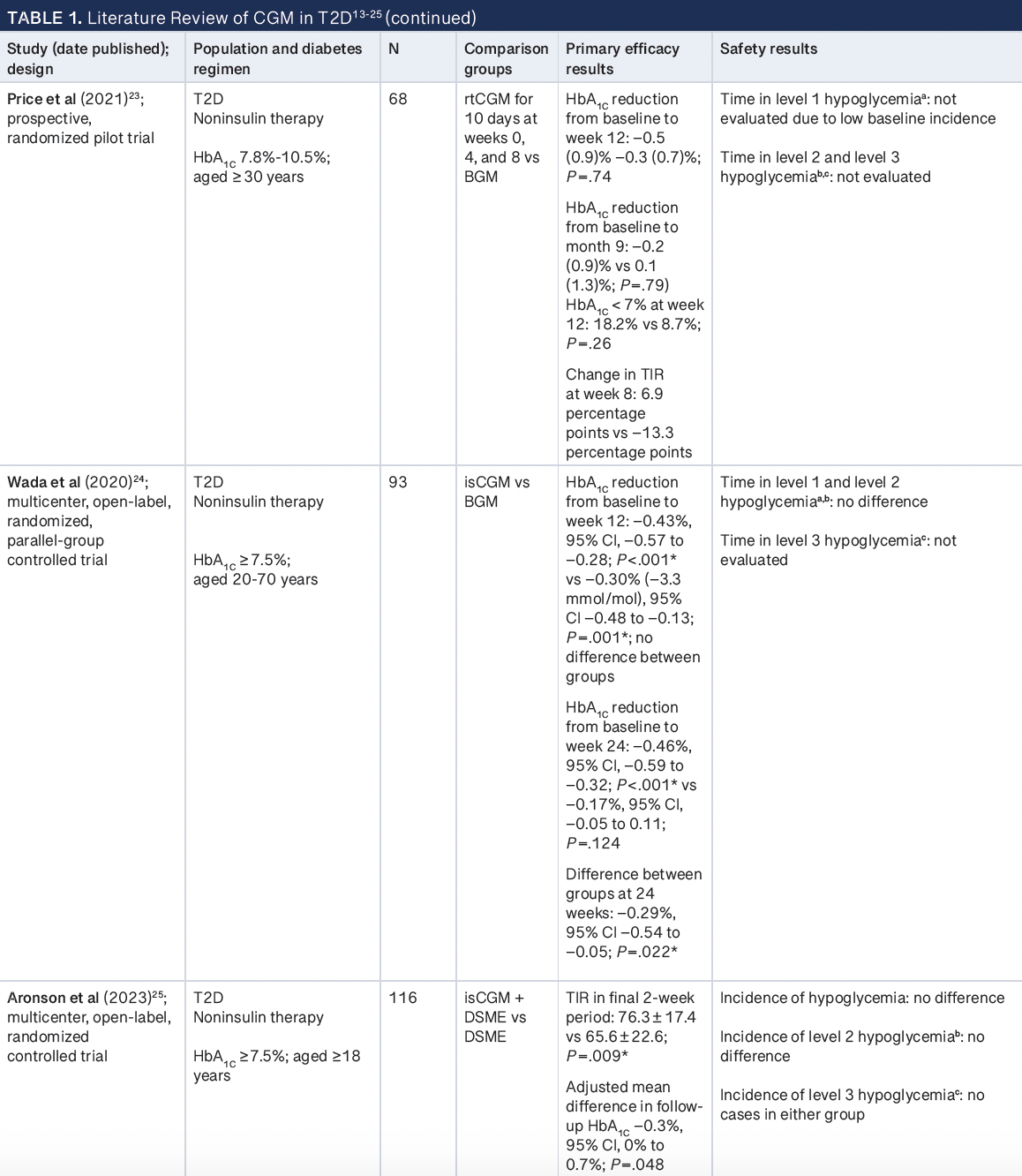
Data regarding the use of CGM specifically in patients using noninsulin therapies for diabetes management only are limited. However, there are studies that suggest a potential benefit. Two studies looked at the impact of episodic CGM use over the course of up to 3 months. Glycemic control improved slightly in those using CGM in both studies, but the effect was not sustained upon CGM discontinuation.22,23 A third study (UMIN000026452) in patients on noninsulin regimens comparing 12 weeks of isCGM with BGM found that both groups had reductions in HbA1C from baseline to 12 weeks. However, those randomly assigned to isCGM had sustained reductions in HbA1C at 24 weeks, whereas those who used standard BGM did not, suggesting a lasting impact of isCGM use on lifestyle choices.24 A final study (NCT04562714) randomly assigned patients to diabetes self-management education (DSME) alone or in addition to isCGM for 16 weeks and found improvements in both HbA1C and TIR in the isCGM group compared with the DSME-only group.25 No differences in hypoglycemia incidence were found in any of the studies assessing CGM use in those using noninsulin therapies only.22-25
Overall, CGM use appears to be associated with improved glycemic control in patients with T2D regardless of what pharmacological therapy they are on. There is also evidence to suggest that CGM use may be associated with a reduction in hypoglycemia in those specifically using intensive insulin regimens. Details regarding the evidence for CGM use in T2D can be found in Table 1.13-25
Advantages of CGM Use
HbA1C is often considered the gold standard for glycemic monitoring as it provides a single laboratory value that represents a 90-day average. Although this test may be considered standard of care across many guidelines and clinical trials, it fails to predict daily glucose fluctuations. Additionally, conditions that affect red blood cell turnover, such as anemia, blood transfusions, human immunodeficiency virus, and kidney disease, may result in falsely elevated or falsely low HbA1C levels. Traditional BGM using finger-stick testing provides a snapshot of BG levels. Despite frequent monitoring, it can miss glycemic variability and identifying glucose patterns from a glucometer or logbook can be difficult and time-consuming. CGM can help improve glycemic control and decrease glycemic variability by reporting numerous readings per day. Additionally, it can help predict trends in glycemic patterns throughout the day and provide information on the time that glucose levels are within, above, and below the goal range.4,26-28 Patients can share their CGM data with health care professionals through portals such as LibreView and Dexcom Clarity, which allow clinicians to make efficient, informed pharmacologic and nonpharmacologic interventions during office visits or televisits.29 Professional-use CGM can provide useful information to clinicians working with patients whose reported BG levels do not correlate with their HbA1C or who may be experiencing asymptomatic hypoglycemia. It can also help providers overcome clinical inertia for patients who are unable to consistently utilize BGM but may not be eligible for insurance coverage for personal-use CGM. Blinded professional-use CGM can give providers insight into a patient’s typical glucose patterns without influencing the patient’s behavior, allowing for appropriate therapy adjustments to be made. Unblinded professional-use CGM can provide the patient with real-time feedback and may prompt the patient to make lifestyle adjustments.30
CGM is also an appealing alternative for patients who are fearful of needles and for patients with severe peripheral neuropathy, as it is minimally invasive and less painful than traditional BGM. It can also be useful in patients with physical barriers to BGM including those with upper extremity amputations and patients with dexterity limitations, as well as those with difficulty obtaining finger-stick blood samples due to various complications. Given the ease of use of CGM, patients can test their glucose levels while out of the house without requiring a private and sanitary space.31 The majority of current CGM devices utilize alarms to notify patients of out-of-range glucose levels in real time.29 While a reading establishes BG levels at 1 point in time, CGM devices can detect the rate of change in levels and predict the risk of hypoglycemia or hyperglycemia. Both features allow a patient to respond accordingly to prevent severe complications and can be particularly useful in patients with frequent episodes of hypoglycemia and in those with hypoglycemia unawareness. Prediction of hypoglycemia may be beneficial for patients who live alone and therefore do not have assistance available to manage a severe hypoglycemic episode. Patients can also choose to share their CGM data with friends, family members, or caregivers through product-specific applications so they receive alerts for out-of-range glucose readings. CGM also provides consistent information regarding the impact of diet, exercise, and stress on glucose levels.32
Limitations of CGM Use
There are several limitations to consider before recommending a CGM device. The initial barrier to CGM is often insurance coverage, as plans have specific eligibility requirements.33 Literature and guidelines clearly support CGM use for those with T1D, so most commercial payers offer coverage.4,6-12 For those with T2D, many commercial payers offer coverage if patients are on MDIs or CSII but may not provide coverage for those on noninsulin therapies.22-24 Copayments and product discounts vary based on commercial insurance and device. Documentation may also be requested to show a patient meets criteria.34,35
Recently, the Centers for Medicare & Medicaid Services (CMS) expanded coverage for CGM devices to include patients with T2D using any type of insulin. Medicare beneficiaries with a history of problematic hypoglycemia now also qualify regardless of their medication regimens. Problematic hypoglycemia is defined as either recurrent level 2 hypoglycemic events (BG level < 54 mg/dL) despite 2 or more attempts to adjust medications or history of a hypoglycemic event during which the patient required third-party assistance for treatment of hypoglycemia (level 3 hypoglycemia).36 For coverage, both a receiver and sensor are required. In the United States, the receiver for the FreeStyle Libre 3 is not commercially available, limiting use in this population.37 On the other hand, some insurance companies will cover CGM sensors but do not cover the receiver. In this case, it is crucial to ensure that a smartphone is compatible with the sensor prior to placement.34,35
If the CGM system is not covered by insurance, a cost-benefit discussion is needed. Patients who accrue copayments from frequent hospitalizations or emergency department visits may be willing to pay for a CGM system out of pocket to improve glycemic management and prevent frequent visits. The cost of the device varies, with each 10- or 14-day personal-use sensor costing approximately $80 to $150.34,35 Clinicians can consider setting these patients up with a professional-use CGM as there is no or limited out-of-pocket cost to most patients.33,34
Once coverage for CGM is confirmed, most patients require extensive education on the application of sensors, receiver use, and appropriate response to alerts and alarms to ensure safe use.38 Additionally, patients must be educated on any substances that can interfere with the accuracy of CGM readings depending on the CGM device (Table 2).4,37,39-45
User error can impact the utility and accuracy of CGM data. For instance, while out-of-range alerts can be useful for safety, an excessive number can cause alert fatigue. Some CGM sensors falsely detect hypoglycemic episodes when compressed, occurring when a sleeping patient’s body exerts pressure on the sensor. This can lead to overtreatment of hypoglycemia if not confirmed with a BG reading.38 If a glucose level is rapidly changing, the CGM will lag behind the true BG level, which can lead to delayed detection of hypoglycemia.46 For this reason, BGM is still required in conjunction with certain CGM devices when glucose levels are rapidly changing, to confirm hypoglycemia or when symptoms do not match the CGM reading. Therefore, all patients should have traditional BGM supplies for the following scenarios: suspicion that CGM is inaccurate, waiting for warm-up, calibrations, if a warning message appears, and when glucose levels are rapidly changing (> 2 mg/dL/min).4
Additionally, patients may experience barriers due to the adhesive on CGM sensors. The sensor may require additional adhesive or an over-patch to secure the device and ensure that it stays on, especially when the patient may sweat. If the sensor falls off, the patient can contact the manufacturer for a replacement. The adhesive may cause contact dermatitis. The site of application should be thoroughly cleaned before application to diminish the risk of dermatitis. Additionally, patients can rotate the CGM insertion site.46
Pharmacists in ambulatory care and community settings can serve as essential resources for patients initiated on CGM to overcome some of the barriers of CGM use. In the ambulatory care setting, pharmacists may have longer and more frequent visits with patients than with other clinicians, so time can be dedicated to comprehensive CGM education at initiation and follow-up visits. When prescribing a CGM device under a collaborative practice agreement (CPA), pharmacists can confirm that patients are prescribed traditional BGM supplies and provide education on when BG levels should be checked. Pharmacists in the community are an accessible resource for patients with questions at the time of CGM device pickup and can identify potential drug or supplement interactions with CGM devices. Although there are challenges associated with CGM devices, pharmacists can play a key role in ensuring that the benefits outweigh the limitations so that patients who qualify for CGM are offered a device.
Differences Among Personal-Use CGMs
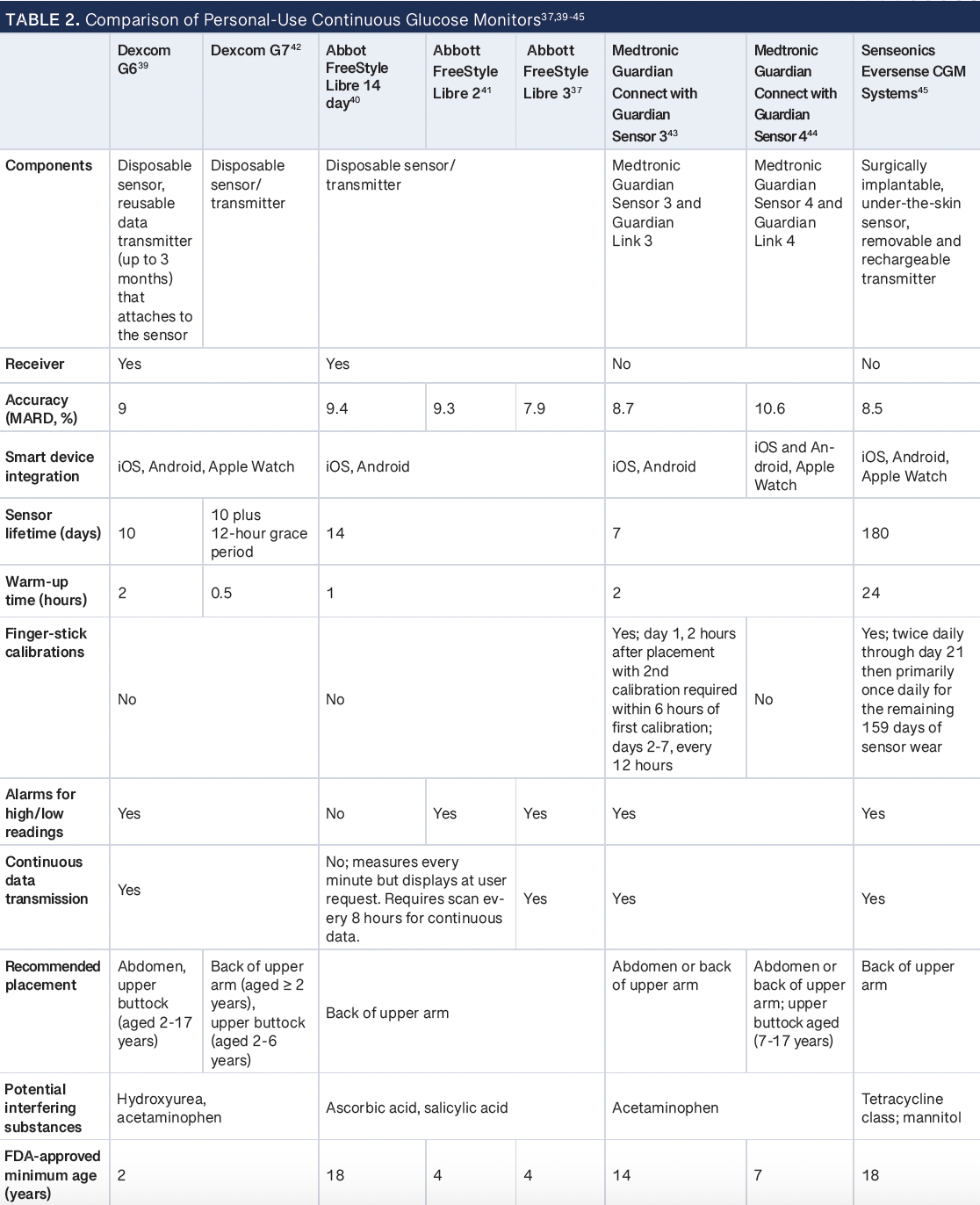
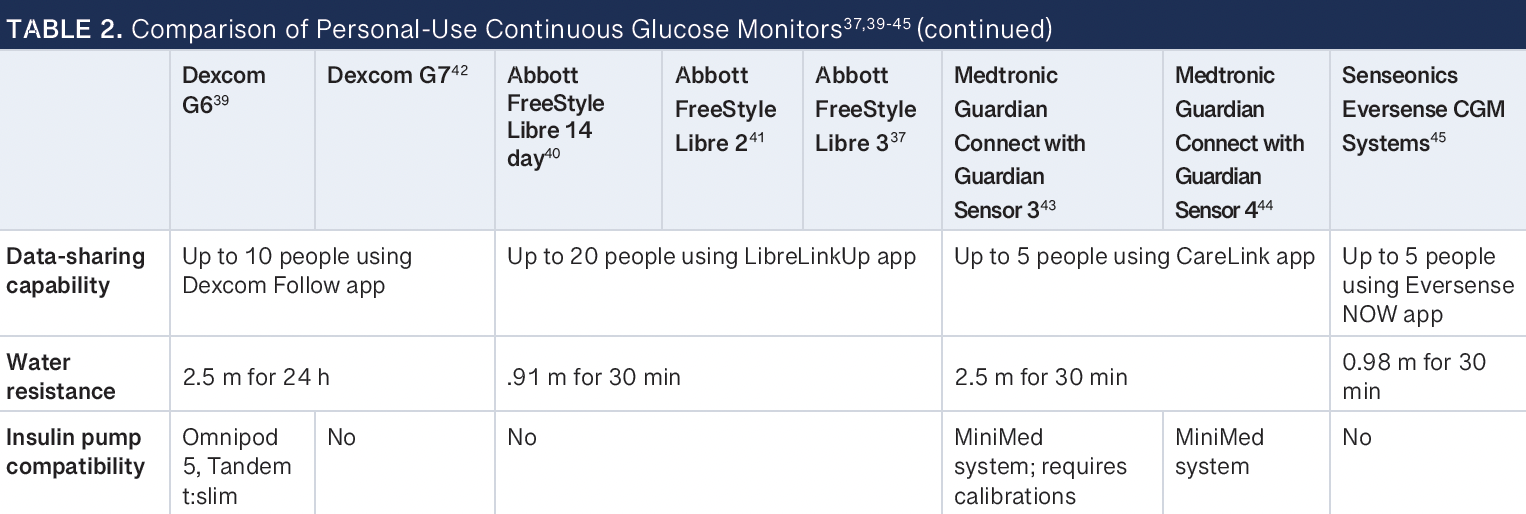
There are currently 8 personal-use CGM devices that are FDA approved: Dexcom G6 and G7, Abbott FreeStyle Libre 14 Day Flash Glucose Monitoring System (FreeStyle Libre 14 day), FreeStyle Libre 2, FreeStyle Libre 3, Medtronic Guardian Connect with Guardian Sensor 3 and 4, and Senseonics Eversense CGM Systems.37,39-45 These devices are owned by the patient and provide unblinded data for real-time clinical decisions. The differences are described in Table 2.37,39-45 Abbott FreeStyle Libre 14 day and Libre 2 are the only isCGMs available. Additionally, Dexcom G7, released in 2023, offers a disposable sensor and transmitter combination product similar to the FreeStyle Libre systems.42 This was a departure from the G6 system that had a separate reusable transmitter and disposable sensor. All systems include trend arrows to prospectively guide treatment decisions. All of the CGM systems except the FreeStyle Libre 14 day include alarms to warn patients of rising or falling glucose levels.40 Alarms and alerts can be adjusted based on individual preference and should align with patient-specific goals. However, the urgent low alarm (glucose level < 55 mg/dL) cannot be disabled on any device. The CGM devices require patients to confirm the alarm to turn it off. Additionally, all patients should remove the sensor before MRI, CT scan, x-ray, or diathermy treatment. If traveling, patients should request an alternative to the full-body scanner.37,39-45
FreeStyle can be worn for up to 14 days. Dexcom CGM devices have a sensor lifetime of 10 days. However, the G7 has an additional 12-hour grace period and the shortest warm-up of 30 minutes compared with 60 to 120 minutes for other available systems.42 Currently, Dexcom G6 and the Medtronic’s Guardian systems are the only CGM devices that have insulin pump compatibility, creating a closed-loop system.39,43,44 All personal-use CGM devices are compatible with a smartphone as the receiver; however, not all smartphone models have specific CGM mobile application capability. It is important for patients to check whether the mobile application is compatible with their device before starting to use a CGM system.
Accuracy of CGM devices is determined by mean absolute relative difference (MARD), which represents the average of the absolute error among all CGM values and matched reference values.47 The smaller the percentage, the greater the accuracy of the CGM device. A MARD of less than 10% is considered clinically accurate for medication adjustments without traditional BG confirmation.48 All current personal-use CGM devices except the Medtronic Guardian 4 system have a MARD less than 10% when placed on the upper arm.44 Of note, both Medtronic Guardian Sensor 3 and Eversense CGM systems recommend daily BG calibrations for accuracy.43,45 Of the personal-use CGM devices on the market, the Dexcom CGM, FreeStyle Libre, and Eversense CGM systems have been FDA approved for medication dosing based on CGM readings.
Differences Among Professional-Use CGMs
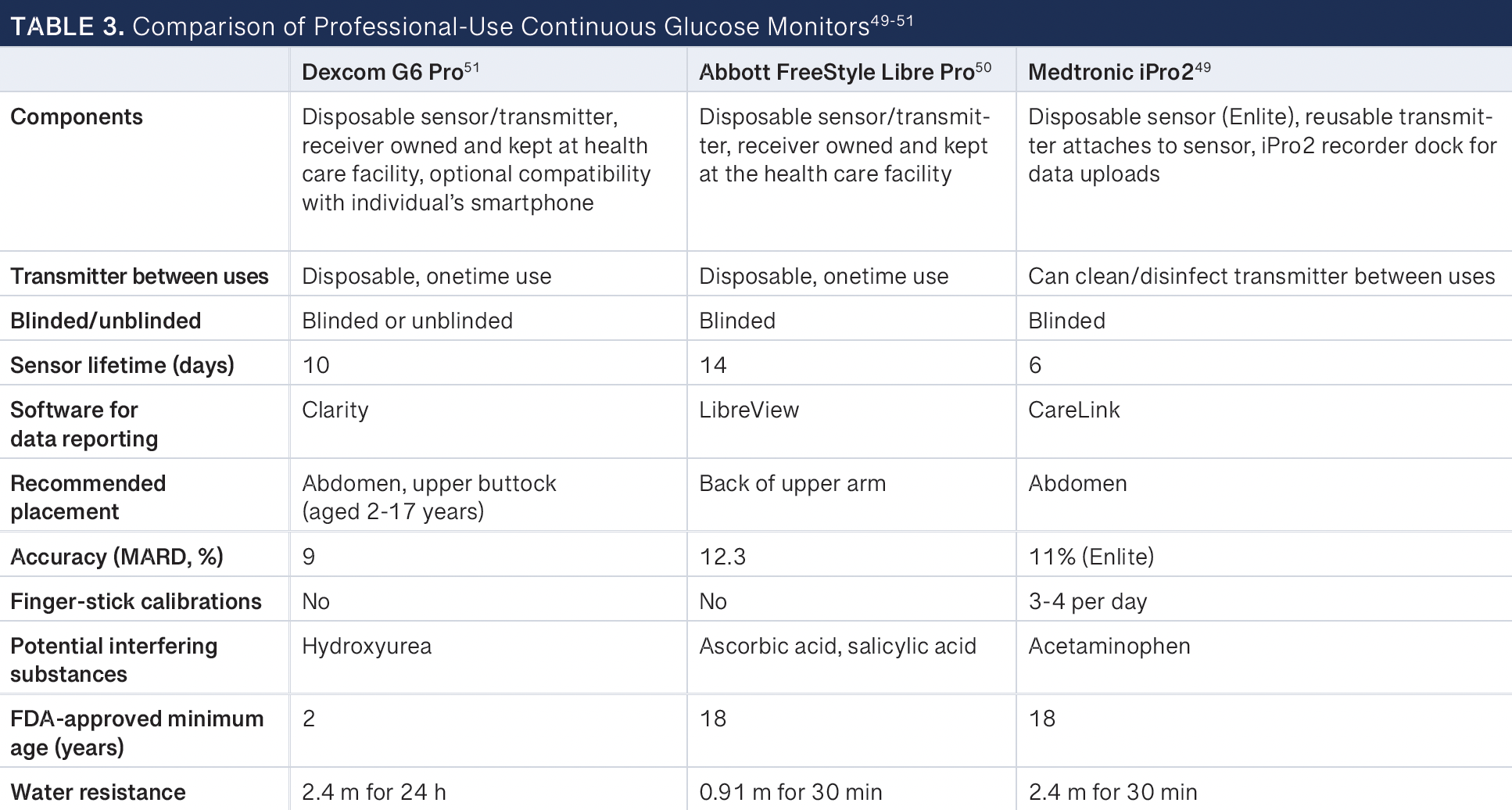
There are 3 professional-use CGM devices commercially available: Dexcom G6 Pro, Abbott FreeStyle Libre Pro, and Medtronic iPro2.49-51 Only the Dexcom G6 Pro allows for both blinded and unblinded data collection and can be used in pediatric patients 2 years and older. The minimum FDA-approved age for Abbott FreeStyle Libre Pro and Medtronic iPro2 is 18 years. Medtronic iPro2 is the only professional CGM device that requires traditional BG calibrations up to 4 times per day. Further comparison among available professional-use CGMs can be found in Table 3.49-51
A pharmacist can help determine which CGM device is best based on patient-specific factors and insurance coverage. Pharmacists can also play a vital role in analyzing CGM data and make or implement recommendations for medication adjustments depending upon the state they are licensed in.
Interpreting Results
Medication management should be done based on the data obtained in the ambulatory glucose profile (AGP) report,4 which is a visualization of data containing an overall glucose median and highlighted areas. The median is represented by a solid line; half of all glucose levels are above and half are below this line. Shaded areas representing the 25th to 75th percentile provide a visual indicator of the degree of glucose variability. Different AGP reports can also include a shaded portion highlighting the 10th to 90th percentile or 5th to 95th percentile of data. The comprehensive information obtained provides pharmacists with a snapshot of data that will help them assess glycemic patterns and make individualized recommendations. Data sufficiency is crucial when interpreting the AGP report. A study conducted by Riddlesworth et al demonstrated that CGM data from the 14-day period prior to HbA1C collection correlated well with HbA1C results and CGM data for the preceding 3 months. It was concluded that having at least 70% or 10 days of CGM usage provided data that were a reliable indicator of usual glycemic patterns.52
AGP reports contain important terminology that pharmacists should become familiar with. These include the glucose management indicator, which reflects the CGM-estimated HbA1C, and TIR, defined as the percentage of time interstitial glucose measures between 70 mg/dL and 180 mg/dL. Studies have shown a correlation between TIR and predicted laboratory-obtained HbA1C, with higher TIR corresponding with lower HbA1C.53 The goal for the majority of patients is a TIR percentage of approximately 70%, which correlates to a predicted HbA1C of 6.9%. Targets are adjusted for pregnant patients; those at high risk of hypoglycemia, such as elderly patients; and patients with less-stringent HbA1C goals. Time above range (TAR) and TBR represent the percentage of readings and time a patient is not at targeted goal. TAR can further be divided into 2 levels: level 1 representing the percentage of readings between 181 mg/dL and 250 mg/dL and level 2 representing the readings greater than 250 mg/dL. TBR level 1 represents the percentage of readings between 54 mg/dL and 69 mg/dL, while level 2 displays readings of less than 54 mg/dL. Lastly , it is important for pharmacists to assess the glycemic variability, which displays the coefficient of variation of glycemic readings. This is calculated from the mean glucose and standard deviation, with stable readings representing a variability of 36% or less. Readings above this value suggest an increased risk of hypoglycemia.
The majority of CGM systems today allow a limited view of recent data to be displayed on the reader/receiver. To obtain the full AGP report, the user must download the reader/receiver to their software or remotely share data with the pharmacist via automatic uploads to the cloud. Full reports will provide day-to-day graphs and allow for an interactive discussion about diet, exercise, adherence, and goals. Pharmacists can register their clinical practice on the software and have patients sign up directly to view reports both in person and remotely. Based on the information collected, they can address any hypoglycemia and optimize pharmacological therapy accordingly.
CGM Billing and Reimbursement
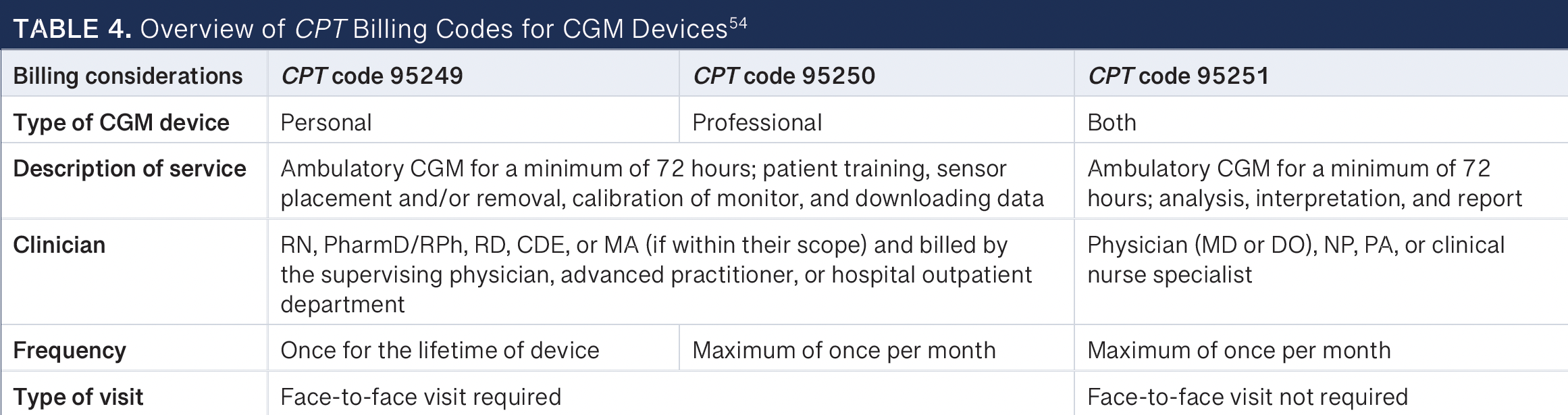
For pharmacists to integrate CGM into their practices, they need to have the resources to bill for their services. Three Current Procedural Terminology (CPT) codes are currently approved for CGM systems: 95249, 95250, and 9525154; 95249 and 95250 are linked to personal-use and professional-use devices, respectively. These codes reimburse for the necessary training, sensor placement, hookup, calibration, sensor removal, and data downloaded. Any trained health care professional, including pharmacists, may provide the service associated with these codes if they are doing so as directed by a physician or other qualified clinician. The code 95249 may be submitted only once unless the patient changes manufacturers or has a different model of data receiver. The code 95251 covers the interpretation and analysis of CGM data. It can be used for any CGM device but is billable only by a physician or licensed nonphysician provider based on individual state law.
The evaluation and management (E/M) codes 99211 to 99215 may be billed on the same day if there was “significant and separately identifiable evaluation and management service performed” and modifier 25 is added to confirm that the E/M service was separate and identifiable from the CGM service. The CGM codes require a minimum of 72 hours of device data to bill.54 Therefore, 95249 or 95250 may be billed the same day as 95251. Additionally, only 95251 may be provided as a non-face-to-face encounter (Table 4).54
Pharmacists can have a financially sustainable role in providing CGM services to patients. In addition to setting up professional-use CGM services, pharmacists can conduct all the services described for codes 95249 and 95250. For code 95251, only a CMS recognized provider may bill the code.
However, a pharmacist practicing under a CPA can analyze and interpret the AGP report and implement recommendations. Additionally, the pharmacist can ensure the elements required for appropriate CGM analysis and interpretation are documented: patient’s name, date of birth, medical record number, indication for the device placement, name and type of device placed, sensor placement and removal date (removal should occur after at least 72 hours), date of downloaded data, analysis and interpretation of data, and signature of interpreting physician or another qualified nonphysician provider. Finally, the correct International Statistical Classification of Diseases, Tenth Revision, diagnosis code must accompany the claim. The national average reimbursement rates for CPT codes 95249 to 95251 and 99211 to 99215 can be found in Table 5.55-57
Conclusion
The ADA and AACE guidelines recommend CGM technology for specific populations of patients with diabetes based upon current literature. There are many advantages to CGM use, such as detailed glucose levels and barriers including insurance coverage. Pharmacists play a significant role in initiating and maintaining patients on CGM devices. Data from CGM devices can then be utilized to optimize pharmacological therapy and help patients achieve their glycemic targets. Lastly, by applying CPT codes, pharmacists can offer and expand the benefits of CGM to patients living with diabetes.
References
About the Authors
Rebecca M. Khaimova, PharmD, BCACP, CDCES, is an ambulatory care clinical pharmacist at One Brooklyn Health – Brookdale.
Rachel L. Quinn, PharmD, BCACP, AE-C, is an ambulatory clinical pharmacist at Shields Health Solutions.
Rachel A. Galbo, PharmD, BCACP, CDCES, is a ambulatory care pharmacist at Mount Sinai Health System.
Anthony M. Gerber, PharmD, BCACP, AAHIVP, is a CDTM ambulatory care clinical pharmacist at New York City Health + Hospital/Bellevue in New York, New York.
1. National diabetes statistics report, 2020. CDC. Accessed January 26, 2024. https://www.cdc.gov/diabetes/pdfs/data/statistics/nationaldiabetes-statistics-report.pdf
2. Clarke SF, Foster JR. A history of blood glucose meters and their role in self-monitoring of diabetes mellitus. Br J Biomed Sci. 2012;69(2):83-93.
3. Nathan DM, Genuth S, Lachin J, et al; Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977-986. doi:10.1056/NEJM199309303291401
4. ElSayed NA, Aleppo G, Aroda VR, et al. 7. Diabetes technology: standards of care in diabetes-2023. Diabetes Care. 2023;46(suppl 1):S111-S127. doi:10.2337/dc23-S007
5. McBane SE, Dopp AL, Abe A, et al; American College of Clinical Pharmacy. Collaborative drug therapy management and comprehensive medication management-2015. Pharmacotherapy. 2015;35(4):e39-e50. doi:10.1002/phar.1563
6. Grunberger G, Sherr J, Allende M, et al. American Association of Clinical Endocrinology clinical practice guideline: the use of advanced technology in the management of persons with diabetes mellitus. Endocr Pract. 2021;27(6):505-537. doi:10.1016/j.eprac.2021.04.008
7. Blonde L, Umpierrez GE, Reddy SS, et al. American Association of Clinical Endocrinology clinical practice guideline: developing a diabetes mellitus comprehensive care plan-2022 update. Endocr Pract. 2022;28(10):923-1049. doi:10.1016/j.eprac.2022.08.002
8. Tamborlane WV, Beck RW, Bode BW, et al; Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med. 2008;359(14):1464-1476. doi:10.1056/NEJMoa0805017
9. Beck RW, Riddlesworth T, Ruedy K, et al. Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections: The DIAMOND randomized clinical trial. JAMA. 2017;317(4):371-378. doi:10.1001/jama.2016.19975
10. Lind M, Polonsky W, Hirsch IB, et al. Continuous glucose monitoring vs conventional therapy for glycemic control in adults with type 1 diabetes treated with multiple daily insulin injections: the GOLD randomized clinical trial. JAMA. 2017;317(4):379-387. doi:10.1001/jama.2016.19976
11. van Beers CA, DeVries JH, Kleijer SJ, et al. Continuous glucose monitoring for patients with type 1 diabetes and impaired awareness of hypoglycaemia (IN CONTROL): a randomised, open-label, crossover trial. Lancet Diabetes Endocrinol. 2016;4(11):893-902. doi:10.1016/S2213-8587(16)30193-0
12. Deiss D, Bolinder J, Riveline JP, et al. Improved glycemic control in poorly controlled patients with type 1 diabetes using real-time continuous glucose monitoring. Diabetes Care. 2006;29(12):2730-2732. doi:10.2337/dc06-1134
13. Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline JP, Rayman G. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther. 2017;8(1):55-73. doi:10.1007/s13300-016-0223-6
14. Ruedy KJ, Parkin CG, Riddlesworth TD, Graham C; DIAMOND Study Group. Continuous glucose monitoring in older adults with type 1 and type 2 diabetes using multiple daily injections of insulin: results from the DIAMOND trial. J Diabetes Sci Technol. 2017;11(6):1138-1146. doi:10.1177/1932296817704445
15. Beck RW, Riddlesworth TD, Ruedy K, et al. Continuous glucose monitoring versus usual care in patients with type 2 diabetes receiving multiple daily insulin injections: a randomized trial. Ann Intern Med. 2017;167(6):365-374. doi:10.7326/M16-2855
16. Martens T, Beck RW, Bailey R, et al. Effect of continuous glucose monitoring on glycemic control in patients with type 2 diabetes treated with basal insulin: a randomized clinical trial. JAMA. 2021;325(22):2262-2272. doi:10.1001/jama.2021.7444
17. Ehrhardt NM, Chellappa M, Walker MS, Foda SJ, Vigersky RA. The effect of real-time continuous glucose monitoring on glycemic control in patients with type 2 diabetes mellitus. J Diabetes Sci Technol. 2011;5(3):668-675. doi:10.1177/193229681100500320
18. Elliott T, Beca S, Beharry R, Tsoukas MA, Zarruk A, Abitbol A. The impact of flash glucose monitoring on glycated hemoglobin in type 2 diabetes managed with basal insulin in Canada: a retrospective real-world chart review study. Diab Vasc Dis Res. 2021;18(4):14791641211021374. doi:10.1177/14791641211021374
19. Carlson AL, Daniel TD, DeSantis A, et al. Flash glucose monitoring in type 2 diabetes managed with basal insulin in the USA: a retrospective real-world chart review study and meta-analysis. BMJ Open Diabetes Res Care. 2022;10(1):e002590. doi:10.1136/bmjdrc-2021-002590
20. Wright Jr EE, Kerr MS, Reyes IJ, Nabutovsky Y, Miller E. Use of flash continuous glucose monitoring is associated with HBA1C reduction in people with type 2 diabetes treated with basal insulin or noninsulin therapy. Diabetes Spectr. 2021;34(2):184-189. doi:10.2337/ds20-0069
21. Yoo HJ, An HG, Park SY, et al. Use of a real time continuous glucose monitoring system as a motivational device for poorly controlled type 2 diabetes. Diabetes Res Clin Pract. 2008;82(1):73-79. doi:10.1016/j.diabres.2008.06.015
22. Moon SJ, Kim KS, Lee WJ, Lee MY, Vigersky R, Park CY. Efficacy of intermittent short-term use of a real-time continuous glucose monitoring system in non-insulin–treated patients with type 2 diabetes: a randomized controlled trial. Diabetes Obes Metab. 2023;25(1):110-120. doi:10.1111/dom.14852
23. Price DA, Deng Q, Kipnes M, Beck SE. Episodic real-time CGM use in adults with type 2 diabetes: results of a pilot randomized controlled trial. Diabetes Ther. 2021;12(7):2089-2099. doi:10.1007/s13300-021-01086-y
24. Wada E, Onoue T, Kobayashi T, et al. Flash glucose monitoring helps
achieve better glycemic control than conventional self-monitoring of blood glucose in non-insulin-treated type 2 diabetes: a randomized controlled trial. BMJ Open Diabetes Res Care. 2020;8(1):e001115. doi:10.1136/bmjdrc-2019-001115
25. Aronson R, Brown RE, Chu L, et al. Impact of flash glucose monitoring in people with type 2 diabetes inadequately controlled with non-insulin antihyperglycaemic therapy (IMMEDIATE): a randomized controlled trial. Diabetes Obes Metab. 2023;25(4):1024-1031. doi:10.1111/dom.14949
26. Benhamou PY, Catargi B, Delenne B, et al. Real-time continuous glucose monitoring (CGM) integrated into the treatment of type 1 diabetes: consensus of experts from SFD, EVADIAC and SFE. Diabetes Metab. 2012;38(suppl 4):S67-S83. doi:10.1016/S1262-3636(12)71538-0
27. Bergenstal RM, Ahmann AJ, Bailey T, et al. Recommendations for standardizing glucose reporting and analysis to optimize clinical decision making in diabetes: the ambulatory glucose profile. J Diabetes Sci Technol. 2013;7(2):562-578. doi:10.1177/193229681300700234
28. Patton S, Clements M. Continuous glucose monitoring versus self-monitoring of blood glucose in children with type 1 diabetes- are there pros and cons for both?. US Endocrinol. 2012;8(1):27-29.
29. Carlson AL, Mullen DM, Bergenstal RM. Clinical use of continuous glucose monitoring in adults with type 2 diabetes. Diabetes Technol Ther. 2017;19(S2):S4-S11. doi:10.1089/dia.2017.0024
30. Shrivastav M, Gibson Jr W, Shrivastav R, et al. Type 2 diabetes management in primary care: the role of retrospective, professional continuous glucose monitoring. Diabetes Spectr. 2018;31(3):279-287. doi:10.2337/ds17-0024
31. Lin R, Brown F, James S, Ekinci E. Continuous glucose monitoring: a review of the evidence in type 1 and 2 diabetes mellitus. Diabet Med. 2021;38(5):e14528. doi:10.1111/dme.14528
32. Cowart K, Updike WH, Franks R. Continuous glucose monitoring in persons with type 2 diabetes not using insulin. Expert Rev Med Devices. 2021;18(11):1049-1055. doi:10.1080/17434440.2021.1992274
33. Kruger DF, Anderson JE. Continuous glucose monitoring (CGM) is a tool, not a reward: unjustified insurance coverage criteria limit access to CGM. Diabetes Technol Ther. 2021;23(S3):S45-S55. doi:10.1089/dia.2021.0193
34. Cost and coverage. FreeStyle Libre. 2024. Accessed January 26, 2024. https://www.freestyle.abbott/us-en/cost.html
35. The Dexcom G7 con tinuous glucose monitoring(CGM) system: pharmacy toolkit. Dexcom. 2023. Accessed May 5, 2023. https://dexcompdf.s3.us-west-2.amazonaws.com/HCP_Website/Pharmacist/LBL-1000964+G7+Pharmacist+Toolkit+PDF+version.pdf
36. Glucose monitors. Centers for Medicare & Medicaid Services. 2024. Accessed February 15, 2024 https://www.cms.gov/medicare-coveragedatabase/view/lcd.aspx?LCDId=33822
37. Nguyen A, White JR. FreeStyle Libre 3. Clin Diabetes. 2022;41(1):127-128. doi:10.2337/cd22-0102
38. Bruttomesso D, Laviola L, Avogaro A, et al. The use of real time continuous glucose monitoring or flash glucose monitoring in the management of diabetes: a consensus view of Italian diabetes experts using the Delphi method. Nutri Metab Cardiovasc Dis. 2019;29(5):421-431. doi:10.1016/j.numecd.2019.01.018
39. Dexcom G6 continuous glucose monitoring system user guide. Dexcom. Updated March 2022. Accessed May 5, 2023. https://s3-us-west-2.amazonaws.com/dexcompdf/G6-CGM-Users-Guide.pdf#page=21
40. FreeStyle Libre 14-day system: getting started guide. Abbott. 2019. Accessed May 5, 2023. https://www.binsons.com/uploads/userfiles/files/documents/products/Libre%2014%20Day%20Getting%20Started%20Guide.pdf
41. FreeStyle Libre 2 Flash Glucose Monitoring System user’s manual. Abbott. Updated June 2020. Accessed May 5, 2023. https://www.binsons.com/uploads/userfiles/files/documents/products/Libre%202%20User%20Manual.pdf
42. G7 user guide. Dexcom. Updated December2023. Accessed February 15, 2024 https://s3.us-west-2.amazonaws.com/dexcompdf/Downloads+and+Guides+Updates/AW00046-05+UG+G7+OUS+en+MMOL.pdf
43. Guardian Sensor (3) user guide. 2018. Medtronic Diabetes. Accessed May 5, 2023. https://www.medtronicdiabetes.com/sites/default/files/library/download-library/user-guides/Guardian-Sensor-3-user-guide.pdf
44. Guardian 4. 2023. Medtronic Diabetes. Accessed November 25, 2023. https://www.medtronicdiabetes.com/sites/default/files/library/download-library/user-guides/Guardian_4_transmitter_user_guide.pdf
45. Eversense user guide. Senseonics. June 4, 2019. Accessed May 5, 2023. https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160048S006c.pdf
46. Maiorino MI, Petrizzo M, Bellastella G, Esposito K. Continuous glucose monitoring for patients with type 1 diabetes on multiple daily injections of insulin: pros and cons. Endocrine. 2018;59(1):62-65. doi:10.1007/s12020-017-1328-z
47. Reiterer F, Polterauer P, Schoemaker M, et al. Significance and reliability of MARD for the accuracy of CGM systems. J Diabetes Sci Technol. 2017;11(1):59-67. doi:10.1177/1932296816662047
48. Danne T, Nimri R, Battelino T, et al. International consensus on use of continuous glucose monitoring. Diabetes Care. 2017;40(12):1631-1640. doi:10.2337/dc17-1600
49. iPro2 user guide. Medtronic Diabetes. 2015. Accessed May 5, 2023. https://www.medtronicdiabetes.com/sites/default/files/library/download-library/user-guides/iPro2_User_Guideen-US.pdf
50. FreeStyle Libre Pro. 2024. Accessed January 26, 2024. https://www.FreeStyle.abbott/in-en/libre-pro.html
51. Dexcom G6 Pro Continuous Glucose Monitoring System user guide. Dexcom. Updated March 2022. Accessed May 5, 2023. https://dexcompdf.s3-us-west-2.amazonaws.com/Dexcom-G6-Pro-User-Guide.pdf
52. Riddlesworth TD, Beck RW, Gal RL, et al. Optimal sampling duration for continuous glucose monitoring to determine long-term glycemic control. Diabetes Technol Ther. 2018;20(4):314-316. doi:10.1089/dia.2017.0455
53. Bergenstal RM. Continuous glucose monitoring data as an adjunct to HBA1C. In: Role of Continuous Glucose Monitoring in Diabetes Treatment. American Diabetes Association; 2018:19-20.
54. AACE guide to continuous glucose monitoring (CGM). American Association of Clinical Endocrinologists. 2023. Accessed May 5, 2023. https://pro.aace.com/cgm/toolkit/billing-codes
55. Overview of the Medicare Physician Fee Schedule search. Centers for Medicare & Medicaid Services. Updated September 8, 2023. Accessed May 5, 2023. https://www.cms.gov/medicare/physician-fee-schedule/search/overview
56. CMS-1772-FC. 2023. Centers for Medicare & Medicaid Services. Accessed May 5, 2023. https://www.cms.gov/medicaremedicare-fee-servicepaymentascpaymentasc-regulations-and-notices/cms-1772-fc
57. Davis JB. Medical Fees Directory: UCR and Medicare Fees with RVUs for Over 9,000 CPT Codes. Practice Management Info; 2022.
The authors have no conflicts of interest to disclose.





 but ≥ 54 mg/dL (3.0 mmol/L). bLevel 2 hypoglycemia: blood glucose concentration < 54 mg/dL (3.0 mmol/L). cLevel 3 hypoglycemia: severe hypoglycemia event requiring assistance from another person. *Significant difference.")

 but ≥ 54 mg/dL (3.0 mmol/L). bLevel 2 hypoglycemia: blood glucose concentration < 54 mg/dL (3.0 mmol/L). cLevel 3 hypoglycemia: severe hypoglycemia event requiring assistance from another person. *Significant difference.")

 but ≥ 54 mg/dL (3.0 mmol/L). bLevel 2 hypoglycemia: blood glucose concentration < 54 mg/dL (3.0 mmol/L). cLevel 3 hypoglycemia: severe hypoglycemia event requiring assistance from another person. *Significant difference.")